The penalties will fall heaviest on hospitals in New Jersey, New York, the
District of Columbia, Arkansas, Kentucky, Mississippi, Illinois and
Massachusetts, a Kaiser Health News analysis of the records
shows. Hospitals that treat the most low-income patients will be hit
particularly hard.
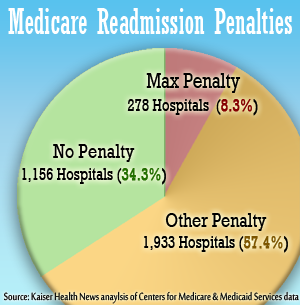
A total of 278 hospitals nationally will lose the maximum amount allowed
under the health care law: 1 percent of their base Medicare reimbursements.
Several of those are top-ranked institutions, including Hackensack University
Medical Center in New Jersey, North Shore University Hospital in Manhasset, N.Y.
and Beth Israel Deaconess Medical Center in Boston, a teaching hospital of
Harvard Medical School.
"A lot of places have put in a lot of work and not seen improvement," said
Dr. Kenneth Sands, senior vice president for quality at Beth Israel. "It is not
completely understood what goes into an institution having a high readmission
rate and what goes into improving" it.
Sands noted that Beth Israel, like several other hospitals with high
readmission rates, also has unusually low mortality rates for its patients,
which he says may reflect that the hospital does a good job at swiftly getting ailing patients back and preventing
deaths.
Penalties Will Increase Next Year
The maximum penalty will increase after this year, to 2 percent of regular
payments starting in October 2013 and then to 3 percent the following year. This
year, the $280 million in penalties comprise about 0.3 percent of the total
amount hospitals are paid by Medicare.
According to Medicare records, 1,933 hospitals will receive penalties less
than 1 percent; the total number of hospitals receiving penalties is 2,211.
Massachusetts General Hospital in Boston, which U.S. News last month ranked as
the best hospital in the country, will lose 0.5 percent of its
Medicare payments because of its readmission rates, the records show. The smallest penalties are one hundredth of a
percent, which 50 hospitals will receive.
Dr. Eric Coleman, a national expert on readmissions at the
University of Colorado School of Medicine, said the looming penalties have
captured the attention of many hospital executives. "I’m not sure penalties
alone are going to move the needle, but they have raised awareness and moved
many hospitals to action," Coleman said.
The penalties have been intensely debated. Studies have found that
African-Americans are more likely to be readmitted than other patients, leading
some experts to be concerned that hospitals that treat many blacks will end up
being unfairly punished.
Hospitals have been complaining that Medicare is applying the rule more
stringently than Congress intended by holding them accountable for returning
patients no matter the reason they come back.
Hospitals That Serve Poor Are Hit Harder Than Others
Some safety-net hospitals that treat large numbers of low-income patients
tend to have higher readmission rates, which the hospitals attribute to the lack
of access to doctors and medication these patients often experience after
discharge. The analysis of the penalties shows that 76 percent of the hospitals
that have a lot of low-income patients will lose Medicare funds in the
fiscal year starting in October. Only 55 percent of the hospitals treating few
poor patients are going to be penalized, the analysis shows.
"It’s our mission, it’s good, it’s what we want to do, but to be penalized
because we care for those folks doesn’t seem right," said Dr. John Lynch, chief
medical officer at Barnes-Jewish Hospital in St. Louis, which is receiving the
maximum penalty.
"We have worked on this for over four years," Lynch said, but those efforts
have not substantially reduced the hospital’s readmissions. He said
Barnes-Jewish has tried sending nurses to patients’ homes within a week of
discharge to check up on them, and also scheduled appointments with a doctor at
a clinic, but half the patients never showed. This spring, the hospital
established a team of nurses, social workers and a pharmacist to monitor
patients for 60 days after discharge.
"Some of the hospitals that are going to pay penalties are not going to be
able to afford these types of interventions," said Lynch, who estimated the
penalty would cost Barnes-Jewish $1 million.
Atul Grover, chief public policy officer for the Association of American
Medical Colleges, called Medicare’s new penalties "a total disregard for
underserved patients and the hospitals that care for them." Blair Childs, an
executive at the Premier healthcare alliance of hospitals, said: "It’s really
ironic that you penalize the hospitals that need the funds to manage a
particularly difficult population."
Medicare disagreed, writing that "many safety-net providers
and teaching hospitals do as well or better on the measures than hospitals
without substantial numbers of patients of low socioeconomic
status." Safety-net hospitals that are not being penalized include the
University of Mississippi Medical Center in Jackson and Denver Health Medical
Center in Colorado, the records show.
Bill Kramer, an executive with the Pacific Business Group on Health, a
California-based coalition of employers, said the penalties provide "an
appropriate financial incentive for hospitals to do the right thing in terms of
preventing avoidable readmissions."
The government’s penalties are based on the frequency that Medicare heart
failure, heart attack and pneumonia patients were readmitted within 30 days
between July 2008 and June 2011. Medicare took into account the sickness of the
patients when calculating whether the rates were higher than those of the
average hospital, but not their racial or socio-economic background.
The penalty will be deducted from reimbursements each time a hospital submits
a claim starting Oct. 1. As an example, if a hospital received the maximum
penalty of 1 percent and it submitted a claim for $20,000 for a stay, Medicare
would reimburse it $19,800.
The Centers for Medicare & Medicaid Services has been trying to help
hospitals and community organizations by giving grants to help them coordinate
patients’ care after they’re discharged. Leaders at many hospitals say they are
devoting increased attention to readmissions in concert with other changes
created by the health law.
Sally Boemer, senior vice president of finance at Mass General, said she
expected readmissions will drop as the hospital develops new methods of
arranging and paying for care that emphasize prevention. Readmissions "is a big
focus of ours right now," she said.
Gundersen Lutheran Health System in La Crosse, Wis., and Intermountain
Medical Center in Murray, Utah, were among 1,156 hospitals where Medicare
determined the readmission rates were acceptable. Those hospitals will not lose
any money. On average, the readmissions penalties were lightest on
hospitals in Utah, South Dakota, Vermont, Wyoming and New Mexico, the analysis
shows. Idaho was the only state where Medicare did not penalize any
hospital.
Even some hospitals that won’t be penalized are struggling to get a handle on
readmissions. Michael Baumann, chief quality officer at the University of
Mississippi Medical Center, said in-house doctors had made headway against heart
failure readmissions by calling patients at home shortly after discharge. "It’s
a fairly simple approach, but it’s very labor intensive," he said.
The problems afflicting many of the center’s patients—including obesity and
poverty that makes it hard to afford medications—make it more challenging. "It’s
a tough group to prevent readmissions with," he said.
Data for individual hospitals are available as a PDF
file and as a CSV
spreadsheet.
jrau@kff.org